
Low-Level Laser (Light) Therapy

BeLanguageSchool
Hello!
Buongiorno! Hej!
Quam arcu vestibulum, quisque sed est vitae. Elit amet tristique sagittis.

Low-Level Laser (Light) Therapy
Alopecia is a common disorder affecting more than half of the population worldwide. Androgenetic alopecia, the most common type, affects 50% of males over the age of 40 and 75% of females over 65. Only two drugs have been approved so far (minoxidil and finasteride) and hair transplant is the other treatment alternative. This review surveys the evidence for low-level laser therapy (LLLT) applied to the scalp as a treatment for hair loss and discusses possible mechanisms of actions.
It has long been known that red or near-infrared laser light promotes tissue repair and regeneration and low-intensity light called low-level laser therapy (LLLT) stimulates cellular activity. After the discovery of lasers in the 1960s, there has been tremendous interest in using these laser devices to treat various medical conditions. The most commonly used devices have wavelengths in the range 500–1,100 nm (the so-called optical window of tissue) and they deliver fluences of 1–10 J/cm2 with a power density of 3–90 mW/cm2. LLLT has shown beneficial effects for a variety of medical conditions such as wound healing, nerve regeneration, joint pain relief, stroke recovery, and the prevention and treatment of mucositis. Home-use LLLT devices that emit low power coherent monochromatic red light have been developed for various skin conditions, including hair growth. In this review, we will focus on the use of LLLT as a potential treatment for several types of hair loss.
0
Teachers in our school
Donec vestibulum justo a diam ultricies pel
0
%
Of satisfied students
Tortor hendrerit elit fermentum consequat
0
New students a year
Penatibus in lobortis venenatis blandit transitat
0
Different halls and rooms
Efficitur si arcu libero aliquet blanden ferment
HAIR AND TYPES OF HAIR LOSS
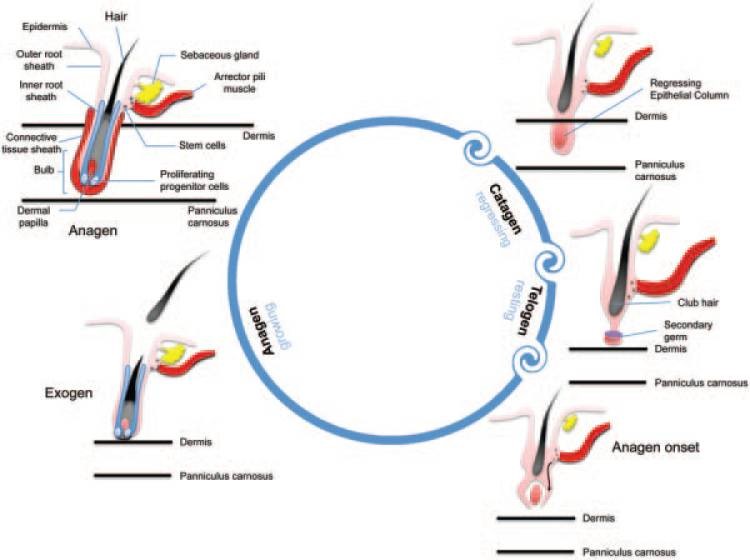
Hair is one of the fastest growing tissues of the human body and the hair follicle, which is a unique characteristic of mammals, represents a stem cell-rich, prototypic neuroectodermal–mesodermal interaction system. Hair follicles undergo repetitive regenerative cycles and each of these cycles consists of three stages: anagen (rapid growth, active stage), catagen (apoptosis-driven regression, physiological involution stage), and telogen (resting stage). Bulge stem cells are found in the region of the outer root sheath located just below the sebaceous gland, coinciding with the point of anchorage of the arrector pili muscle. During the telogen to anagen transition, there is a tightly controlled activation of these epithelial bulge stem cells and within the same period, secondary hair germ cells give rise to transient amplifying (TA) progeny cells. Throughout the entire anagen phase, there is a robust proliferation of the TA cells within the epithelial matrix of the hair follicle. Consequently, proliferating trichocytes terminally differentiate to form the bulk of the hair filament which is the final product of the hair cycle. The dermal papilla of the hair follicle is believed to be the key regulatory element in progenitor cell activation, hair matrix cell proliferation and terminal differentiation of trichocytes.
Androgenetic alopecia (AGA) is the most common form of hair loss in men affecting almost 50% of the male population . AGA refers to hair loss in genetically susceptible individuals caused by effects of androgens such as testosterone and its derivative dihydrotestosterone (DHT). Testosterone is a lipophilic compound that diffuses across the cell membrane.Testosterone is converted by the cytoplasmic enzyme 5-α reductase to DHT, which is its more active form. There are two types of 5-α reductase; Type 1 is found in keratinocytes, fibroblasts, sweat glands, and sebocytes, and Type 2 is found in skin and the inner root sheath of hair follicles. DHT binds the nuclear androgen receptor which regulates gene expression. Disruption of epithelial progenitor cell activation and TA cell proliferation due to abnormal androgen signaling forms the essential pathophysiological component of this condition which in turn leads to continuous miniaturization of sensitive terminal hair follicles, and their conversion to vellus hair follicles.
Although the exact genes involved in hair loss are not clearly known, some of the proposed genes responsible for hair growth are desmoglein, activin, epidermal growth factor (EGF), fibroblast growth factor (FGF), lymphoid-enhancer factor-1 (LEF-1), and sonic hedgehog. As of today, the most common methods used for treating AGA are topical minoxidil, finasteride (males only), and surgical hair transplantation. Unfortunately, current therapies are not efficacious for all patients with AGA. Medical therapies require indefinite use and are limited by patient adherence; surgical options (hair transplants) are limited by cost, each patient’s supply of donor hair, and possible scarring in donor sites. Due to a need for more efficacious therapies, LLLT has emerged as a new therapeutic approach to treat AGA. The Hairmax Lasercomb® was approved by the US Food and Drug Administration (FDA) and received 510 K clearance as a safe therapy for the treatment of male AGA in 2007 and female AGA in 2011 . There has been a recent review on the use of lasers and light therapies for alopecia that covered 308 nm excimer laser, fractional photothermolysis, and UV phototherapy, but did not cover LLLT mediated by red laser which is the main subject of the present review

There are several other forms of hair loss such as alopecia areata (AA), telogen effluvium (TE), and chemotherapy-induced alopecia. AA is an autoimmune inflammatory condition, which presents with non-scarring alopecia and is characterized on histology by intra- or perifollicular lymphocytic infiltrates composed of CD4+ and CD8+ T-cells. There are severe variants of AA: alopecia totalis, a total loss of scalp hair and alopecia universalis, total loss of scalp and body hair. The most common treatment modality is intralesional corticosteroid injections; however, other treatments include topical and systemic corticosteroids, minoxidil, anthralin, contact sensitizers, psoralen plus ultraviolet A, cyclosporine, tacrolimus, and biologics such as alefacept, efalizumab, etanercept, infliximab, and adalimumab. TE is abnormal hair cycling causing excessive loss of telogen hair. Some common causes include acute severe illness, surgery, iron deficient anemia, thyroid disease, malnutrition, chronic illness, and medications such as oral contraceptives, lithium, and cimetidine. Chemotherapy works by destroying rapidly dividing cancer cells, however, at the same time, other rapidly dividing cells of the body such as hair follicles are also destroyed, and this unwanted effect leads to chemotherapy-induced alopecia starting 1–3 weeks and peaking at 1–2 months of treatment.
![]()
Mon – Fri:
010:00 AM – 07:00 PM
Sat-Sun:
010:00 AM – 08:00 PM
![]()
Rajmundry: +91-9912327333
Vizag: +91-9912328666
Hyderabad:+91-8977626911
![]()